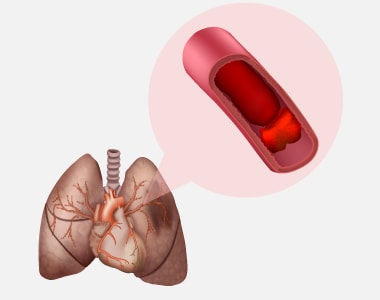
Peripheral arteries are the blood vessels that deliver blood to the lower limbs. When the cholesterol accumulates in these blood vessels, the blood flow to the lower limbs gets blocked. Peripheral angioplasty is a minimally invasive procedure. It is done to restore the blood flow by opening the blocked peripheral arteries.

When is peripheral angioplasty performed?
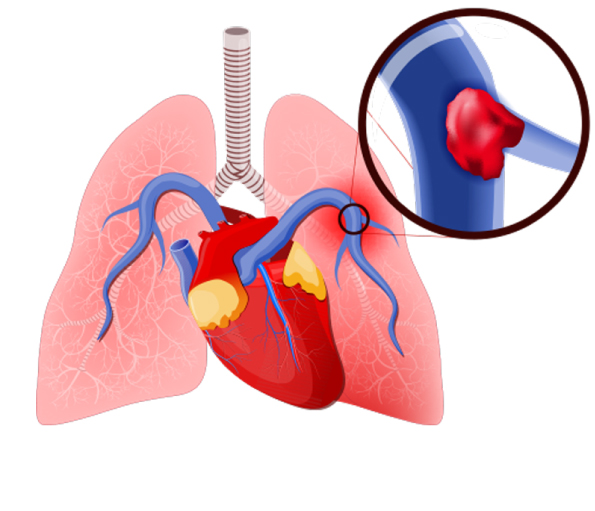
- Peripheral angioplasty is mostly indicated in the treatment of Peripheral Vascular Disease (the circulatory disorder caused by the blocked or narrowed blood vessels outside the heart).
- Peripheral artery disease is the common condition, in which peripheral angioplasty is recommended.
Are there any risks with peripheral angioplasty?
Peripheral angioplasty is associated with the following risks:
- Breathing problems
- Bleeding
- Blood clots
- Infection
- Kidney damage
- Damage to the blood vessel
How to prepare for the procedure?
Before initiating the procedure, a physical examination and imaging tests are done to determine the overall health condition. Additionally, the following steps would help in a successful procedure and quicker recovery:
- Inform the use of current medications, vitamin or mineral supplements.
- Tell the doctor about any underlying disease condition.
- Take the prescribed medicines.
- Notify the doctor if you have any allergies.
- Six to eight hours before the surgery do not eat or drink anything.
What happens during the procedure?
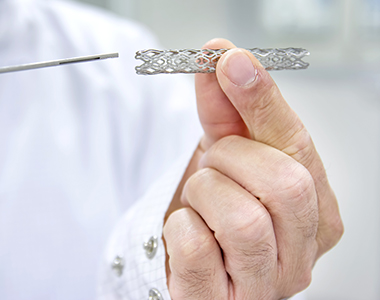
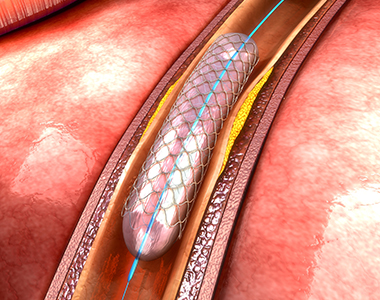
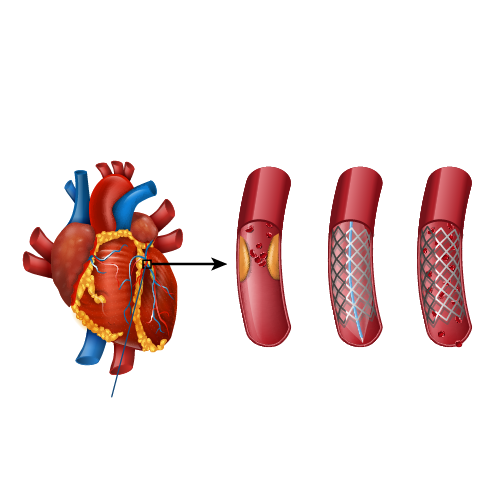
Local anaesthesia is administered in the upper thigh region. Once the anaesthesia sets, an incision is made on the upper thigh to insert the catheter. By using a high-resolution fluoroscopic, the catheter is guided to the blocked artery. When the catheter reaches the obstructed artery, the balloon is inflated to widen the blood vessel. Once the blood flow is restored, a stent is placed to prevent the risk of further blockage. Finally, the incision is closed and covered with a sterilized bandage.
What to expect after the procedure?
You will be placed in a recovery room and the vital parameters would be checked. For at least 3-6 hours, you need to remain still, to prevent bleeding from the incision site. Depending on the patient’s condition, the doctor will decide whether the person requires a hospital stay or not.
Before discharge, you will receive the following instructions:
- Keep the wound clean and dry.
- Do not lift heavyweights.
- Avoid strenuous exercises for at least 24 hours after the procedure.
- Drink plenty of fluids to help flush out the contrast dye from the body.
Care after peripheral angioplasty:
Although peripheral angioplasty clears the blockage, it does not treat the underlying cause of the blockage. So, to prevent the further risk of blockage, the following steps should be taken:
- Maintain a healthy body weight.
- Quit smoking.
- Exercise regularly.
- Take the prescribed medicines to prevent re-narrowing of the blood vessels.
- Manage stress.
- Avoid fatty-foods.
- Have a low-salt and low-fat diet to prevent the risk of fluid retention.
Seek medical attention:
The following symptoms are the warning signs that require immediate medical attention:
- Swelling in limbs
- Chest pain
- Shortness of breath
- Fever associated with chills (over 101oF)
- Weakness
- Dizziness