Congenital heart diseases are diseases that are present from birth and affect the normal heart functioning. These are the most frequently occurring congenital disorder, responsible for 28% of all congenital birth defects. The birth prevalence of CHD is reported to be 8-12/1000 live births. Considering a rate of 9/1000, about 1.35 million babies are born with CHD each year globally.
What are the Causes of Congenital Heart Defects?
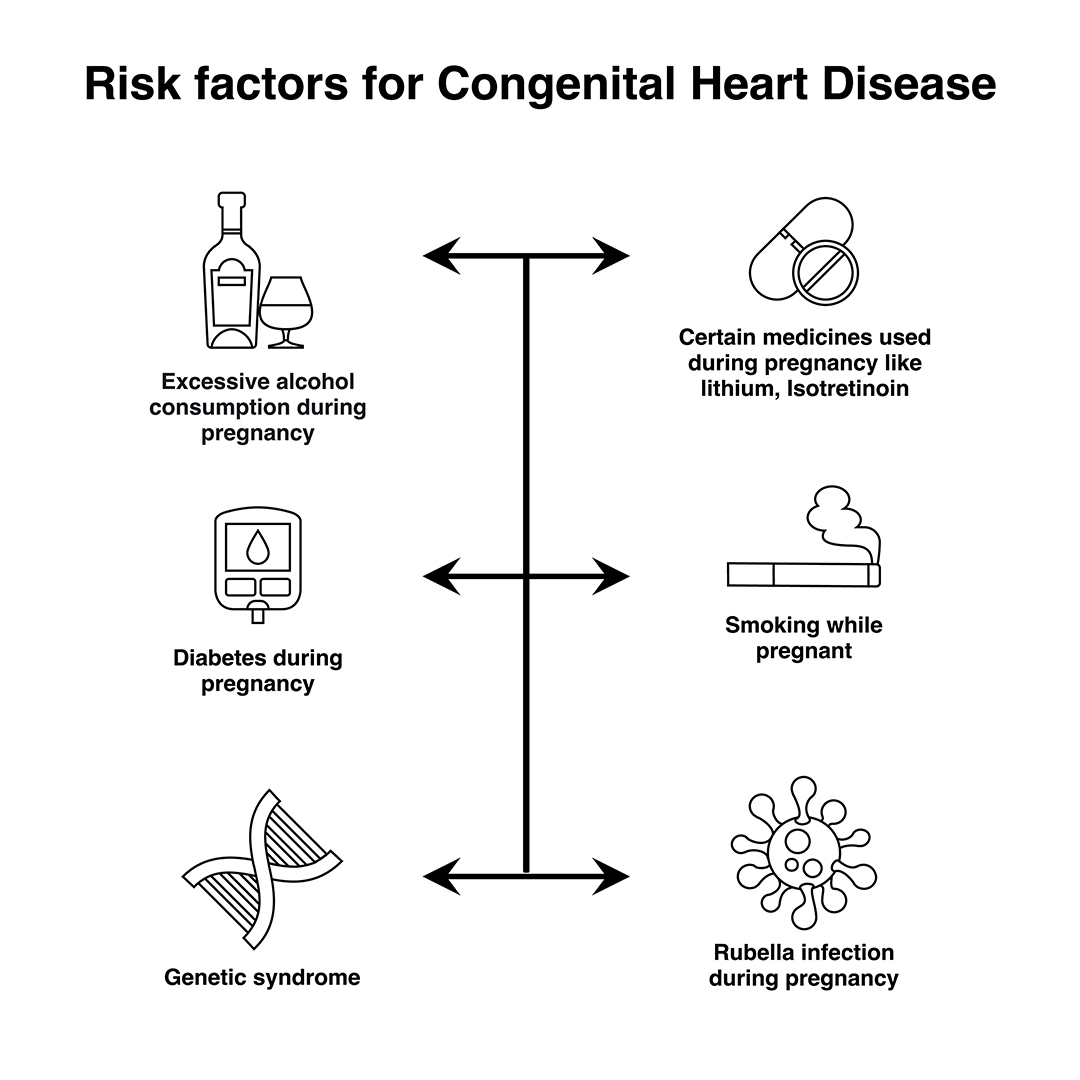
In most cases, no obvious cause of congenital heart disease is identified. However, some things are known to increase the risk of the condition, including:
Down’s syndrome – a genetic disorder that affects a baby’s normal physical development and causes learning difficulties
the mother having certain infections, such as rubella, during pregnancy
the mother taking certain types of medicine during pregnancy, including statins and some acne medicines
the mother smoking or drinking alcohol during pregnancy
the mother having poorly controlled type 1 diabetes or type 2 diabetes
other chromosome defects, where genes may be altered from normal and can be inherited (run in the family)
Many cases of congenital heart disease can be diagnosed before a baby is born during an ultrasound scan in pregnancy. At times a focused foetal heart scan called foetal echocardiography in specialized centers helps to diagnose the cardiac problem before birth. However, it’s not always possible to detect congenital heart defects in this way.
Signs and Symptoms of Congenital Heart Disease
Congenital heart disease can have a number of symptoms, particularly in babies and children, including:
Rapid heartbeat
Rapid breathing
Swelling of the legs, tummy or around the eyes
Extreme tiredness and fatigue
A blue tinge to the skin or lips (cyanosis)
Tiredness and rapid breathing when a baby is feeding
These problems are sometimes noticeable soon after birth, although mild defects may not cause any problems until later in life.
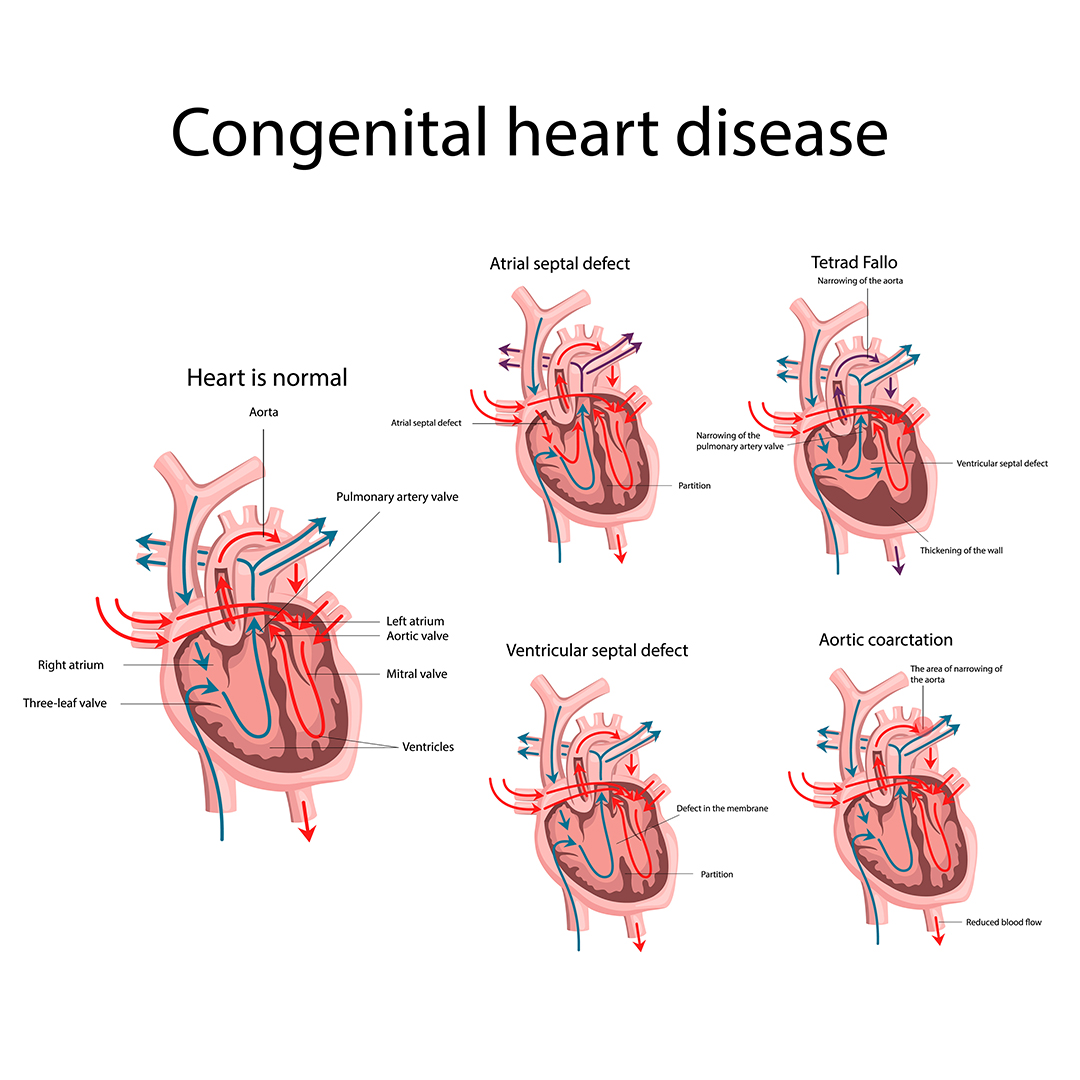
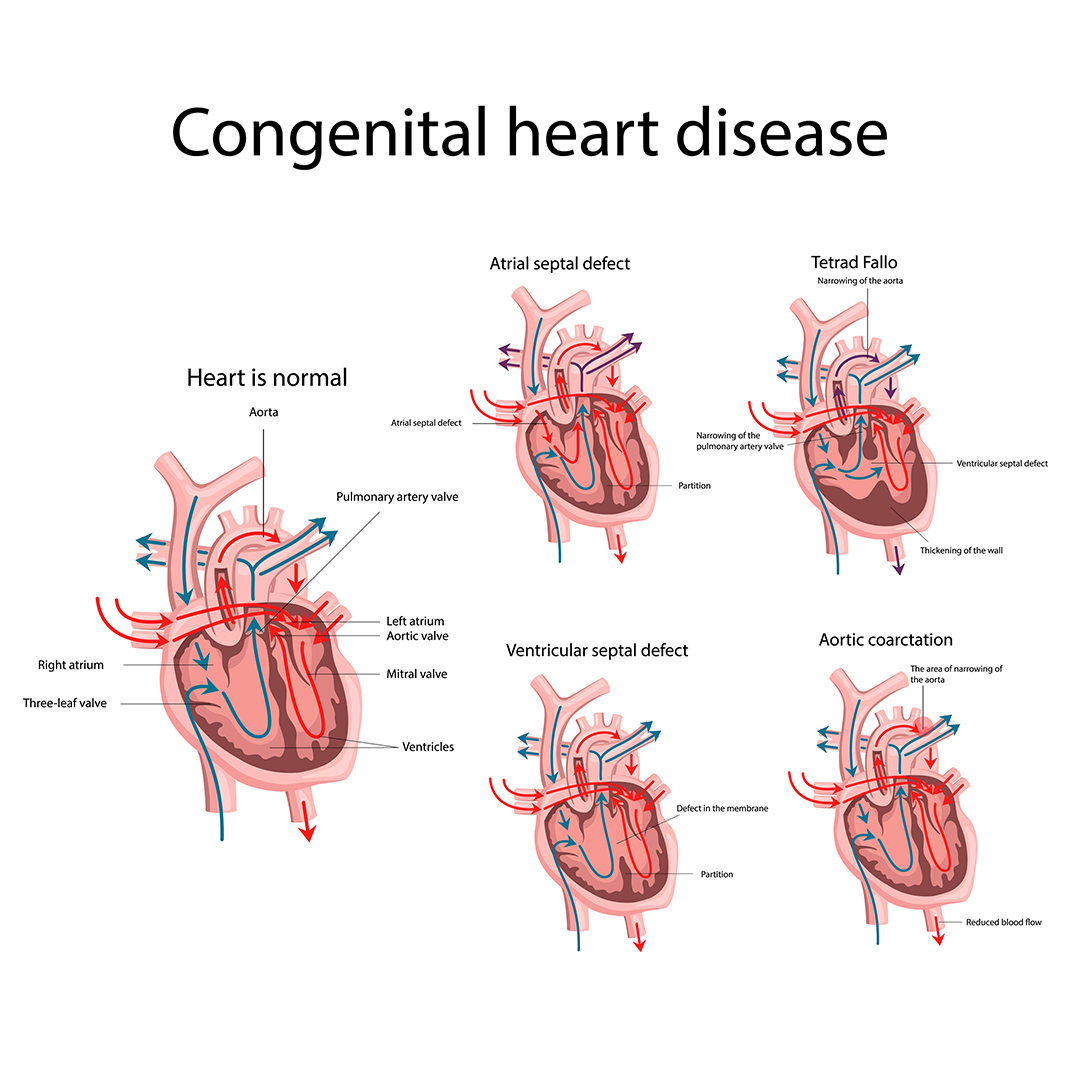
Types of Congenital Heart Disease
There are many types of congenital heart disease and they sometimes occur in combination. Some of the more common defects include:
Septal defects – where there’s a hole between 2 of the heart’s chambers (commonly referred to as a “hole in the heart”)
Coarctation of the aorta – where the main large artery of the body, called the aorta, is narrower than normal
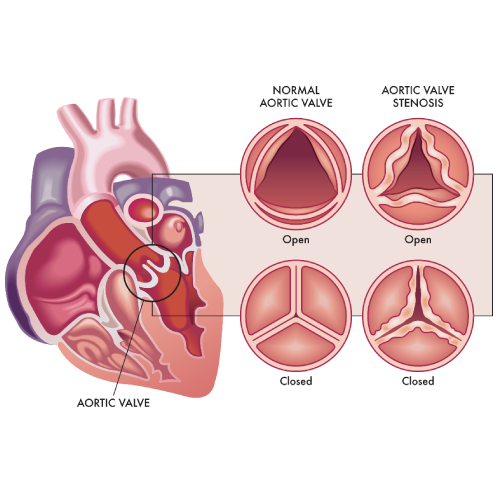
Pulmonary valve stenosis – where the pulmonary valve, which controls the flow of blood out of the lower right chamber of the heart to the lungs, is narrower than normal
Transposition of the great arteries – where the pulmonary and aortic valves and the arteries they’re connected to have swapped positions
Underdeveloped heart – where part of the heart doesn’t develop properly making it difficult for it to pump enough blood around the body or lungs.
Treating Congenital Heart Disease
Treatment for congenital heart disease usually depends on the defect you or your child has.
Mild defects, such as holes in the heart, often don’t need to be treated, as they may improve on their own and may not cause any further problems.
Surgery or interventional procedures are usually required if the defect is significant and causing problems. Modern surgical techniques can often restore most or all of the heart’s normal function.
However, people with congenital heart disease often need treatment throughout their life and therefore require specialist review during childhood and adulthood. This is because people with complex heart problems can develop further problems with their heart rhythm or valves over time.
Most surgery and interventional procedures aren’t considered to be a cure. The affected person’s ability to exercise may be limited and they may need to take extra steps to protect themselves from getting infections.
It’s important that a person with heart disease and their parents or carers discuss these issues with their specialist medical team.
An atrial septum is a muscular wall that separates the upper chambers of the heart called atria. An ASD is a common congenital heart disease where the septum is not formed properly producing a left-to-right shunt, which leads to mixing of oxygenated and deoxygenated blood. This causes pulmonary hypertension and right heart enlargement.
What are the treatment options for ASD?
Small atrial defects do not need any treatment and close on its own. Even in adulthood small ASDs may remain asymptomatic. Some large defects that persists in adulthood may become symptomatic and need closure. The ASDs can be closed by:
Percutaneous closure using a device
Closure through open heart surgery
Percutaneous device closure is the preferred treatment for certain defects type.
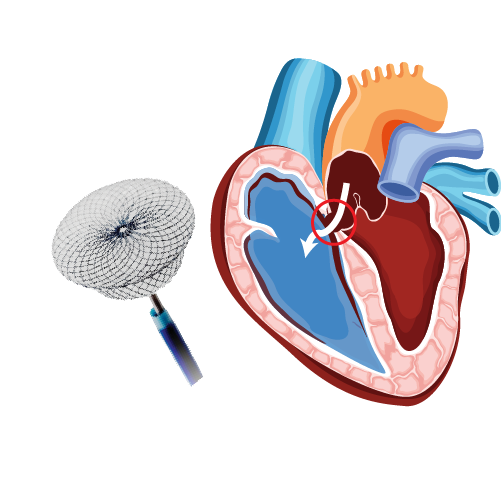
What is Percutaneous Closure of Atrial Septal Defect (ASD)?
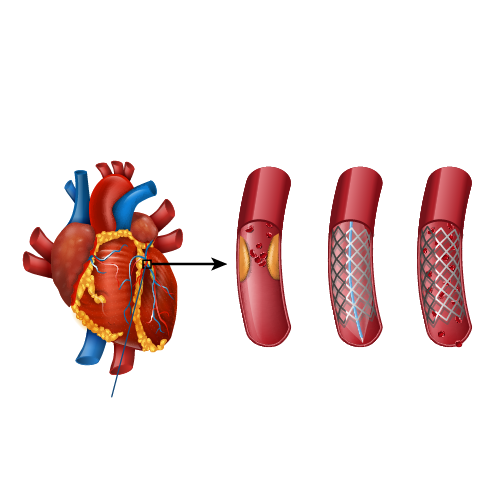
A noninvasive procedure known as percutaneous transcatheter approach is considered depending on the size and severity of the defect. Moderate to large-sized ASD along with pulmonary hypertension requires to be closed. The procedure is performed by inserting a special closure device either folded or attached to a catheter into the vein of the leg and is advanced to the heart through the defect, which closes the hole by a special mechanism.
Are there risks associated with the procedure?
The success rate of the procedure is about 95%. But the risks involved, and their estimated incidence of occurrence include:
Device dislodgement leading to emergency heart surgery: 1%
Device erosion (device eroding through the heart walls): 0.3%
Death: less than 1% usually due to perforation of the heart chamber
Dislodgement of clot or air bubbles to the brain leading to other organs: less than 1%
Arrhythmia: 1 to 2%
Allergic dye reaction
Anaesthetic reaction
Injury to the artery/vein/nerves in the groin
Perforation of the oesophagus
Infection
Allergic reaction to the nickel component of the device
Patients with small ASD may not develop any complications, but large-sized defects may lead to serious complications which demands surgery and prolonged hospitalization.
What is the pre-procedure work-up?
Pre-operative tests to assess the general health of the patient include:
Chest x-ray
Electrocardiogram
Blood tests
Kidney function
A detailed diagnosis of the defect should be performed which includes transthoracic and transoesophageal echocardiogram used to assess the size, location and the suitability of the procedure.
How should I prepare for the procedure?
Patients wearing dentures, glasses or a hearing assist device can plan to wear them during the procedure.
Patient will be instructed about dietary restriction to be followed before the procedure.
Are there any specific instructions about medications?
The healthcare provider may ask you to stop certain medications, such as warfarin or other blood thinners.
If diabetic, consult the physician about how the medication needs to be adjusted.
Provide information about specific allergies regarding iodine, shellfish, X-ray dye, latex or rubber products etc.
What happens during the procedure?
The patient might be asked to have a shower before the procedure.
The patient is asked to wear a hospital gown and lie on an X-ray table where an X-ray camera will move over the chest during the procedure.
Arrangements for intravenous administration of medications or fluids during the procedure will be made.
The site where the catheter will be inserted is cleaned and sterile drapes were used to cover the site to prevent the infection.
Electrodes will be placed on the chest and are attached to an electrocardiograph monitor (ECG).
A sedative might be given to relax, and a local anesthetic is given to numb the site of catheter introduction.
A plastic sheath will be inserted in the groin, through which a catheter is inserted and threaded to the heart.
The physician may also inject a dye which may make you feel hot or flushed for several seconds. Inform the doctor if there is an allergic reaction like itching or tightness in throat, nausea and chest discomfort.
The X-ray cameras are used to obtain the measurements of pressures and oxygen content in the chambers.
The appropriate size and the location of the closure might be visualized using a small catheter connected with an ultrasound transducer.
A special catheter is used to advance the device into the heart and through the defect.
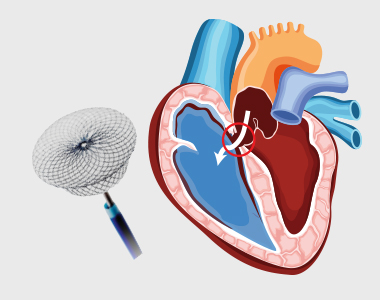
The device is slowly pushed out of the catheter allowing each side of the device to open and close each side of the hole in the septum.
The proper position of the device is ensured and is released from the catheter.
It may take 1-2 hours for the procedure, but preparations must be made to spend about 5-9 hours in the hospital.
The patient should be accompanied by someone who can drive him home, as the patient will not be allowed to drive on the same day.
What care should be taken after the procedure?
The catheter and the imaging probe are removed after the completion of the procedure.
Pressure on the incision site or occasionally a small suture is used to close the vein.
Bed rest is advised for several hours to prevent bleeding, but call the doctor if you notice any bleeding.
You might be advised to drink plenty of water to wash out the contrast material from the body.
Your heart rate and rhythm are monitored; you may be asked to stay overnight in the hospital.
Medications, such as aspirin are prescribed to prevent blood clots.
Strenuous activity and heavy lifting should be avoided for at least six months.
Antibiotic prophylaxis is required for at least six months or lifelong to prevent endocarditis, as per doctor’s advice.
Mitral stenosis is a form of valvular heart disease caused by the narrowing of the mitral valve. Mitral valve lies between the left atrium and left ventricle of the heart which is made up of two flaps of tissue called leaflets. It opens when the blood flows from left atrium and left ventricle and closes immediately to prevent the backward flow of the blood. The defective valve fails to either open or close completely.
The most common cause of mitral stenosis is an infection called rheumatic fever. It is an inflammatory condition that usually starts with strep throat and leads to permanent damage of heart valves. Rheumatic fever is now rare in developed countries, but the prevalence is still high in developing countries. It may scar the mitral valve and if left untreated, mitral stenosis may lead to severe heart complications. Mitral stenosis can be classified into three types – mild, moderate and severe depending on the severity.
Symptoms:
The progression of is slow, and the symptoms generally appear after 20 to 40 years after an episode of rheumatic fever. However, an individual with mitral stenosis may feel fine or have minimal symptoms for decades. They include:
Shortness of breath, especially during physical effort or when you lie down
Chest discomfort or chest pain
Fatigue and weakness, especially during increased physical activity and during pregnancy
Swollen feet or legs
Heart palpitations – sensations of a rapid, fluttering heartbeat
Dizziness or fainting
Coughing up blood
Thromboembolic complications such as stroke
Mitral stenosis symptoms may worsen due to any activity that can cause an increase in the heart rate. The pressure which is built up in the heart due to mitral stenosis causes fluid buildup in the lungs. The symptoms of mitral stenosis usually appear between ages of 15 to 40 years. But they can appear in any age or even during childhood.
The signs that can be found during general examination include:
Heart murmur observed using stethoscope during clinical examination
Fluid buildup in the lungs
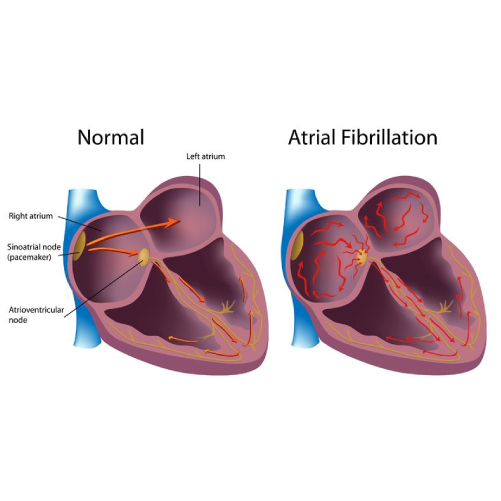
Irregular heart rhythms (arrhythmias)
Causes:
Rheumatic fever: The major cause of mitral stenosis is rheumatic fever. Rheumatic fever is a complication of strep throat which can damage mitral valve by thickening or fusing the valves.
Other causes include:
Calcium deposits: People of older age can develop calcium deposits. This leads to calcification of the mitral valve leaflets resulting in mitral valve stenosis.
Congenital heart disease: Some babies may be born with a narrowed mitral valve, that may lead to mitral stenosis.
Risk factors:
The individuals with the following conditions are at risk of mitral stenosis:
Infective endocarditis
Endomyocardial fibroelastosis
Malignant carcinoid syndrome
Systemic lupus erythematosus
Whipple disease
Rheumatoid arthritis
Diagnosis:
The diagnosis of mitral stenosis could follow an invasive or non-invasive method.
The noninvasive procedures include:
Electrocardiogram (ECG): In this procedure, the electrodes are attached to pads on patients’ skin to measure electrical impulses from the heart which provides information about heart rhythm. The patient is either made to walk on a treadmill or pedal a stationary bike during an Electrocardiogram (ECG) to see how the heart responds to exertion.
Echocardiogram: The echocardiogram is a very useful tool to assess the mitral stenosis etiology, morphology, severity, and treatment intervention.
Two types of echocardiogram are performed which include:
Transthoracic echocardiogram: This test is used to confirm the diagnosis of mitral stenosis. In this procedure, the sound waves are directed to patients’ heart from a transducer held near the chest which produces video images of heart in motion.
Transesophageal echocardiogram: In this procedure a small transducer is attached to the end of a tube which is inserted into esophagus. This provides a closer look at the mitral valve when compared to regular echocardiogram.
Chest X-ray: The chest X-ray is used to observe the size of the heart size, prominent main pulmonary arteries, dilatation of the upper pulmonary veins, and displacement of the esophagus by an enlarged left atrium. If the condition is severe there could be enlargement of all the chambers, pulmonary arteries, and pulmonary veins. The chest X-ray also helps to identify the condition of lungs.
The invasive procedures include:
Cardiac catheterization: Cardiac catheterization is an invasive procedure and is performed when the noninvasive tests are inconclusive or when there is a no correlation between noninvasive tests and clinical findings. It involves threading a thin tube (catheter) through a blood vessel in the patients arm or groin to the coronary artery in the heart and injecting dye through the catheter to make the artery visible on an X-ray. This provides a detailed picture of your heart.
These cardiac tests help in distinguishing mitral valve stenosis from other heart conditions, including other mitral valve conditions. These tests also help reveal the cause of your mitral valve stenosis and whether the valve can be repaired.
Prevention:
The patients with mild mitral stenosis without any symptoms generally do not require an immediate treatment, but are monitored continuously. Medications are prescribed to ease the workload of the heart and to regulate its rhythm, thus reducing the symptoms. The following medications may be prescribed:
Diuretics to reduce fluid accumulation in the body or lungs
Blood thinners (anticoagulants) such as daily intake of aspirin to help prevent blood clots
Beta blockers or calcium channel blockers to slow your heart rate and allow your heart to fill more effectively
Antibiotics to prevent a recurrence of rheumatic fever if it is an underlying cause for the condition
The Treatment Involves Surgical or Nonsurgical Procedures
Nonsurgical procedures:
Percutaneous balloon mitral valvuloplasty
In this procedure, which is also called balloon mitral valvotomy, a soft, thin tube (catheter) tipped with a balloon is inserted in an artery of the patients arm or groin and guided into the narrowed valve. Once in position, the balloon is inflated to widen the valve, improving the blood flow. The balloon is then deflated, and the catheter with balloon is removed.
Surgical options include:
Commissurotomy: An open-heart surgery is performed to remove calcium deposits and other scar tissues to clear the valve passageway.
Mitral valve replacement: Mitral valve replacement is considered if it cannot be repaired. In mitral valve replacement, the damaged valve is removed and is replaced with a mechanical valve or a biological tissue valve.
Prevention:
The prevention of mitral stenosis is largely dependent on preventing the occurrence of rheumatic fever, which is the major cause of the condition. However, if one acquires rheumatic fever, the following measures can help live a healthy life.
Limit intake of salt.
Maintain a healthy body weight.
Decrease caffeine intake.
Seek prompt medical attention.
Cut back on alcohol.
Perform regular exercise.
Go for regular checkups.
MITRAL VALVE DISEASE – Mitral Stenosis( in Telugu)